A. Purpose of the Integrated Plan
The Behavioral Health Services Act (BHSA) requires counties to submit three-year Integrated Plans (IPs) (WIC section 5963) for Behavioral Health Services and Outcomes. Whereas the Three-Year Program and Expenditure Plan required under the Mental Health Services Act (MHSA) focused exclusively on MHSA dollars, the BHSA establishes the IP to serve as a three-year prospective global spending plan that describes how county behavioral health departments plan to use all available behavioral health funding, including BHSA, 1991 and 2011 Realignment, federal grant programs, federal financial participation from Medi-Cal, opioid settlement funds, local funding, and other funding to meet statewide and local outcome measures, reduce disparities, and address the unmet need in their community. In accordance with the BHSA, the IP provides a description of how counties will plan expenditures across a range of behavioral health funding sources and deliver high-quality, culturally responsive, and timely care along the Behavioral Health Care Continuum for the plan period (WIC section 5963, subdivision (a)(1)). The Department of Health Care Services (DHCS) is developing an IP Template, which will include the required elements for each county to submit in their IPs. A copy of the IP Template will be released in this policy manual to inform county planning. Counties will submit the IP through a DHCS web-based county portal.
IPs require counties to conduct a thorough data-informed local service planning process and provide transparency into county planning for expending BHSA funding and all other behavioral health funding sources overseen by counties. All BHSA services and programming must be planned in accordance with local data. In particular WIC section 5963.02, subdivision (b)(2) requires the county to use local substance use disorder (SUD) prevalence data and unmet SUD needs data. IPs will also facilitate local and statewide data collection by providing baseline data on services and planned expenditures and supporting analysis of county goals and outcomes.
A.1 Reporting Period
A draft IP will be due on March 31 for each three-year IP submission. The draft must have a letter from the County Administrative Officer (CAO) approving the draft IP, including the exemption and transfer requests. A final IP is due no later than June 30. County board of supervisor approval is required for submission by June 30 (WIC section 5963.02, subdivision (a)(3)). The board of supervisors is also required to confirm in each IP that the county will meet their realignment obligations (WIC section 14197.71, subdivision (c)(2)). The board of supervisors will attest that the county is meeting their realignment obligations, including but not limited to time and distance standards and appointment time standards as set forth WIC section 14197.7 without utilizing waitlists, through the Behavioral Health Outcomes, Accountability, and Transparency Report (BHOATR) (see Chapter 4 of this policy manual for BHOATR requirements). DHCS will post each county’s IP on the DHCS website.
A.2 Contents of Integrated Plan
The IP Template requires counties to report planned activities and projected expenditures for all county behavioral health department services provided under the following funding sources, services, and programs (WIC section 5963.02, subdivision (c)):
-
Bronzan-McCorquodale Act (1991 Realignment)
-
2011 Realignment
-
Medi-Cal behavioral health programs, including:
-
Specialty Mental Health Services (SMHS)
-
Drug Medi-Cal (DMC)
-
Drug Medi-Cal Organized Delivery System (DMC-ODS)
-
-
Federal block grants, including:
-
Community Mental Health Services Block Grant (MHBG)
-
Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG)
-
Projects for Assistance in Transition from Homelessness (PATH) grant
-
-
BHSA funds
-
Any other federal, state, or local funding directed towards county behavioral health department services, including:
-
Commercial/private insurance
-
Opioid settlement funding (only funds received by the County Behavioral Health Department)
-
County general fund
-
Grant revenue
-
Other
-
The IP Template will include required sections on the following topics:
-
County Demographics and Behavioral Health Needs
-
Plan Goals and Objectives
-
Community Planning Process
-
Comment Period and Public Hearing
-
County Behavioral Health Care Continuum Capacity
-
Services by Total Funding Source
-
Behavioral Health Services Fund Programs
-
Workforce Strategy
-
Budget and Prudent Reserve
A.3 Annual Updates and Intermittent Updates
A.3.1. Purpose of the Annual Updates and Intermittent Updates
Counties use Annual Updates (AUs) and Intermittent Updates (IUs) to respond to changes in local needs during the three-year period for which counties report projections in the IP cycle (“IP period”). Counties will be required to update their IPs through AUs in the second and third years of the IP period (WIC section 5963.03, subdivision (c)). To prepare an AU, counties will review all sections of the IP including the budget template and make revisions for the upcoming fiscal year. DHCS may use AUs to introduce new or revised sections of the IP. Counties may, but are not required to, prepare IUs to their IP at any time during the three-year IP period to report changes that will impact their IP, including ensuring expenditures are consistent with the county’s IP and Budget (WIC section 5963.03, subdivision (c)(1)).
After a county submits its AU or IU, and DHCS approves it, the county’s IP is updated, and becomes the new source document.
DHCS will monitor county implementation of the IP through the corresponding BHOATR and compliance reviews. DHCS will review differences in county performance as projected in the IP, AU, or IU— whichever is the most current for the reporting period— compared to what is reported in the BHOATR for the reporting year.
For example:
-
The first final BHOATR, due January 30, 2029, will focus on FY 2026-2027 and DHCS will use the original final IP, due June 30, 2026, as the baseline for assessing county performance compared to the BHOATR. If a county submits an IU during FY 2026-2027, DHCS will review differences between the BHOATR and the revised IP, which includes changes from the IU.
-
The second BHOATR, due January 30, 2030, will focus on FY 2027-2028 and DHCS will use the AU submitted by June 30, 2027 as the baseline for assessing county performance compared to the BHOATR. If a county submits an IU during FY 2027-2028, DHCS will review differences between the BHOATR and the revised IP.
DHCS will publish the AU and IU template for reference and counties will submit responses via the County Portal.
A.3.2 Annual Update Requirements
Counties will submit draft AUs to DHCS by March 31 prior to the fiscal year the update will cover. The draft must have a letter from the CAO approving the AU. The final AU is due no later than June 30 and requires an approval letter from the County Board of Supervisors approving the AU.
Counties will complete and submit the AU through the County Portal, using the most recently approved IP, AU, or IU as the starting point for edits. County submission for AUs and IUs will follow the same process as outlined above for the IP (See Chapter 3, Section E.4.1 for additional details on submitting via the County Portal). In their AUs, counties can only submit updates for the upcoming fiscal year of the IP period. For example, the Year 2 AU (due by June 30, 2027) can only include projections for the FY 2027-2028 (Year 2) and will not include updates to projections for FY 2028-2029 (Year 3) nor any changes that occurred in FY 2026-27 (Year 1).
Counties will review each IP question and response when completing their AU for the upcoming fiscal year. For questions and responses that do not require changes, the county will resubmit the information provided in the original IP as part of the update. For questions that do require changes, such as changes to the budget template and changes to services offerings, the county will update responses. For example, an AU could indicate that the county is training more behavioral health practitioners in ACT/FACT and IPS than originally anticipated and therefore is increasing the projected number of ACT/FACT teams and IPS teams they will staff for FY 2027-2028. In this example, the county would also update the budget template for Year 2, but would not include any updates for Year 1 and Year 3.
Counties cannot update their exemption requests and funding transfer requests from the original IP without demonstrating to DHCS that they are experiencing a state or local emergency and receiving approval from DHCS to change their requests. See Chapter 6, Section B.5.1 for more information on funding allocation percentage changes.
Counties will request changes to funding allocation percentage changes through their AU in two steps:
-
Step 1: If a county wants to update the funding allocation percentages, they must submit a request to DHCS via the County Portal to open these sections as part of their AU.
-
Step 2: After receiving DHCS permission to update a funding allocation percentage, the county will submit the updates and supporting documentation in the County Portal via the AU.
New AU Questions
During the first IP period, the Year 2 AU (draft due March 31, 2027; final due June 30, 2027) will include new questions related to:
-
Performance measures (“Phase 2 measures”) for the 14 Statewide Behavioral Health Goals.
o Counties must articulate any changes to their approaches for improving performance and addressing disparities on the priority and county-selected optional statewide behavioral health goals, including any adjustments to their approach or services informed by the performance measures available to counties by September 30, 2026. Counties may change their optional goal in the Year 2 AU.
o Beginning with the first AU, counties will use the latest available performance measures to inform planning for future IPs and AUs. Available performance measures must be used in community planning processes and support data-driven decision making for resource allocation and quality improvement.
-
FSP Presumptive Eligibility, as required by AB-348 Full-Service Partnerships (2025) which amended Section 5887 of the Welfare and Institutions Code (more policy guidance on this topic will be provided in future Module releases).
-
Other topics requiring updates, as determined by DHCS.
During the first IP period, the Year 3 AU (draft due March 31, 2028; final due June 30, 2028) will include new questions related to:
-
Additional Performance measures for the Statewide Behavioral Health Goals.
-
Other topics requiring updates, as determined by DHCS.
A.3.3 Intermittent Update (IU) Requirements
Counties may provide urgent updates on information in any allowable sections of the IP by submitting an IU. Counties will submit the IU through the County Portal, using the IP or most recent AU as the starting point for edits. (See Chapter 3, Section E.4. for additional details on submitting via the County Portal). Counties do not need to resubmit sections of the IP that have not changed in IUs.
For example, a county may choose to submit an IU if the county experienced a wildfire, which substantially affected the county’s housing stock. In this instance, the county may need to re-allocate funding from one Housing Intervention to another Housing Intervention to address the crisis. The county would make this change in both the IP narrative section and the budget template. If the county needs to transfer funding from FSP or BHSS into Housing Interventions, they will need to request permission from DHCS to do so (see below). A county is not required to seek approval from DHCS to re-allocate funding between programs under the same BHSA component. However, if the county needs to transfer funding from FSP or BHSS into Housing Interventions, the county needs to obtain approval from DHCS due to the emergency.
Policies for updating exemption requests and funding transfer requests through IUs are the same as the policies for AUs (see the process outlined above in this policy manual Chapter 3, Section A.3.2).
IUs will update the IP or AU (whichever is most recent) to become the new revised IP (i.e., updated IP) and will be in effect in the fiscal year the request is made, upon approval by DHCS. The revised IP will be used as the starting point for the next AU.
A.4 Summary of IP, AU, and IU Requirements
Table A.4.1 Reporting Periods for Integrated Plans, Annual Updates, and Intermittent Updates
|
|
Integrated Plan |
Annual Updates |
Intermittent Updates |
|
Counties are Required to Complete and Submit (WIC section 5963.02, subdivision (a)(1)) |
Yes |
Yes |
If changes are requested |
|
Submission Timeframe |
Every 3 years |
Second and third years of IP period |
Counties may submit at any time during the 3-year IP period |
|
Submission Deadline for Draft (WIC section 5963.02, subdivision (d)) |
Draft due March 31 of year prior to fiscal years IP covers |
Draft due March 31 of year prior to fiscal year annual update covers |
N/A |
|
Behavioral Health Director Certification Required (WIC section 5963.02, subdivision (c)(11)) |
Yes, for draft and final IP Submissions |
Yes, for draft and final AU submissions |
Yes, for final IU submission |
|
County Administrative Officer Letter Required |
Yes, for draft IP submissions |
Yes, for draft annual update submissions |
No |
|
Community Planning Process Required (WIC section 5963.03, subdivision (a)(1)-(2); WIC section 5963, subdivision (c)(2)(A)) |
Yes |
No, but encouraged |
No, but encouraged |
|
30-day Public Comment Period Required (WIC section 5963.03, subdivision (a)(2)(B; WIC section 5963.03, subdivision (c)(2)(B)) |
Yes |
Yes |
Yes |
|
Behavioral Health Board Hearing Required (WIC section 5963.03, subdivision (b)) |
Yes |
If county engages stakeholders |
If county engages stakeholders |
|
Board of Supervisors Approval and Submission (WIC section 5963.02, subdivision (a)(3)) |
Yes, for final IP, by June 30 |
Yes, for final AU, by June 30 |
Yes, submitted at any time in FY |
|
Funding Transfer Requests |
Yes |
No, unless county has DHCS permission |
No, unless county has DHCS permission |
|
Exemption Requests |
Yes |
No, unless county has DHCS permission |
No, unless county has DHCS permission |
B. Community Planning Process
B.1 Stakeholder Involvement
Stakeholder engagement requirements (WIC section 5963.03) for the Integrated Plan (IP) are effective January 1, 2025. Counties must engage with local stakeholders (WIC section 5963.03, subdivision (a)(1)) to develop each element of their IP. The stakeholders that must be engaged) include, but are not limited to:
-
Eligible adults and older adults (individuals with lived experience)
-
Families of eligible children and youth, eligible adults, and eligible older adults (families with lived experience)
-
Youths (individuals with lived experience) or youth mental health or substance use disorder organizations
-
Providers of mental health services and substance use disorder treatment services
-
Public safety partners, including county juvenile justice agencies
-
Local education agencies
-
Higher education partners
-
Early childhood organizations
-
Local public health jurisdictions
-
County social services and child welfare agencies
-
Labor representative organizations
-
Veterans
-
Representatives from veterans’ organizations
-
Health care organizations, including hospitals
-
Health care service plans, including Medi-Cal managed care plans (MCPs) as defined in WIC section 14184.101, subdivision (j)
-
Disability insurers (a commercial disability insurer that covers hospital, medical or surgical benefits as defined in INS section 106, subdivision (b))
-
Tribal and Indian Health Program designees established for Medi-Cal Tribal consultation purposes
-
The five most populous cities in counties with a population greater than 200,000
-
Area agencies on aging
-
Independent living centers
-
Continuums of care, including representatives from the homeless service provider community
-
Regional centers
-
Emergency medical services
-
Community-based organizations serving culturally and linguistically diverse constituents
In addition to the required stakeholders listed above, stakeholders shall include participation of individuals representing diverse viewpoints (WIC section 5963.03, subdivision (2)(A)(ii)), including, but not limited to:
-
Representatives from youth from historically marginalized communities
-
Representatives from organizations specializing in working with underserved racially and ethnically diverse communities
-
Representatives from LGBTQ+ communities
-
Victims of domestic violence and sexual abuse
-
People with lived experience of homelessness
Counties are required to demonstrate a partnership with constituents and stakeholders throughout the process that includes meaningful stakeholder involvement on mental health and substance use disorder policy, program planning and implementation, monitoring, workforce, quality improvement, evaluation, health equity, evaluation, and budget allocations (WIC section 5963.03, subdivision (2)(A)(i)). Meaningful stakeholder engagement requires that counties conduct a community planning process that is open to all interested stakeholders and that stakeholders have opportunities to provide feedback on key planning decisions. Stakeholder engagement should not be limited to individuals who belong to organizations or advocacy groups.
Counties must demonstrate a partnership with constituents and stakeholders (WIC section 5963.03, subdivision (2)(A)(i)) as part of their community planning processes. Examples of meaningful partnership with stakeholders may include, but are not limited to, the following types of stakeholder engagement:
-
Education and engagement to support meaningful involvement, including on policies that govern the behavioral health delivery system
-
Listening sessions
-
Conference calls
-
Client advisory meetings
-
Consumer and family group meetings
-
Town hall meetings
-
Video conferences
-
Media announcements
-
Targeted Outreach
-
Public comment
-
Public hearings
-
Stakeholder workgroups and committees
-
Focus groups
-
Surveys
-
Key informant interviews or engaging with subject matter experts
-
Training, education, and outreach related to community planning
-
Other strategies that demonstrate meaningful partnerships with stakeholders
To ensure that the community planning process is adequately staffed, the county may designate positions and/or units responsible for:(
-
The overall community planning process.
-
Coordination and management of the community planning process.
-
Ensuring that stakeholders have the opportunity to meaningfully and sufficiently participate in the community planning process (WIC section 5963.03, subdivision (2)(A)).
Training should be provided by the county as needed to their staff designated responsible for any of the functions that will enable staff to establish and sustain a community planning process.
A county may also provide supports, including, but not limited to, training and technical assistance, to ensure stakeholders, including peers and families, receive sufficient information and data to meaningfully participate in the development of Integrated Plans and annual updates.
Counties may allocate up to 5 percent of the total annual revenue received from the local Behavioral Health Services Fund (BHSF) to fund planning costs (WIC section 5892, subdivision (c)). For additional information on how counties can fund the community planning process, please refer to the County Planning Funds Chapter 3, Section B.4.
B.2 Considerations of Other Local Program Planning Processes
This section focuses on the requirements for Integrated Plan (IP) development related to collaboration with Medi-Cal Managed Care Plans (MCPs) and local health jurisdictions (LHJs). Per HSC section 124030, subdivision (f) a “Local health jurisdiction” means county health department or combined health department in the case of counties acting jointly or city health department within the meaning of HSC section 101185. Specifically, the Behavioral Health Services Act (BHSA) requires that each county must:
-
Work with its LHJ on the development of its Community Health Improvement Plan (CHIP) (WIC section 5963.01, subdivision (b)); and consider the CHIP of each LHJ that covers residents of the county in preparing their IP and annual update (WIC section 5963.02, subdivision (b)(4)).
-
Work with each MCP that covers residents of the county on the development of the MCP’s Population Needs Assessment (PNA) (WIC section 5963.01, subdivision (a)) and consider the PNA of each MCP that covers residents of the county in preparing their IP and annual update (W&I Code section 5963.02, subdivision (b)(3)).
-
The BHSA was written prior to the 2024 DHCS redesign of PNA requirements. MCPs no longer develop and submit a PNA to the Department of Health Care Services (DHCS). MCPs now fulfill their PNA requirement by meaningfully participating in the Community Health Assessments (CHA) and CHIPs conducted by LHJs. For more information, please see CalAIM: Population Health Management (PHM) Policy Guide. Given these changes, the term local planning is used to describe these PNA requirements.
-
DHCS is focused on building bridges across public health, MCPs, and behavioral health delivery systems. The BHSA transforms the Mental Health Services Act (MHSA) planning process into a broader county and regional planning process. The targeted points of integrations of BHSA community planning processes with the community- and population-level assessment and planning efforts led by public health with MCPs and other stakeholders will reduce siloes and increase cross-system collaboration to enable strategic alignment of funding for coordinated and complementary approaches. DHCS’ goal is to improve upstream interventions and health outcomes for, and thus more effectively improve the lives of, community members. The CalAIM PHM Policy Guide defines upstream interventions include those that link to public health and social services and support members staying healthy through wellness and prevention services.
While perspectives and focus areas may vary, local public health, MCPs, and counties serve common communities, and local integration and partnerships are essential to paving a path toward better understanding the needs of local communities, strategizing appropriate interventions, addressing social determinants of health, and advancing health equity. With this goal in mind, in January 2024, DHCS coordinated with the California Department of Public Health (CDPH) and issued a new policy requiring MCPs to meaningfully participate in LHJ local planning processes, as detailed further below. As the BHSA was written prior to this policy change, this guidance explains the BHSA IP requirements in the context of these other recent policy developments.
This guidance addresses requirements for counties’ IP submissions, specific to collaboration with MCPs and LHJs on Community Health Assessments (CHAs) and CHIPs, to promote greater alignment among public health, managed care, and behavioral health.
B.2.1. Local Planning Overview
This section provides background on MCP and LHJ local planning processes.
B.2.1.1 Background: LHJ, CHA and CHIP
As part of its local planning processes, most LHJs develop both a CHA and a CHIP, which emphasize participatory and collaborative practices centered on the community. For further details and additional context, see the California Department of Public Health December 26, 2023 Memo to All Local Health Jurisdictions and p. 8 – 10 of the CalAIM PHM Policy Guide.
-
The CHA describes the status of population health within a jurisdiction. Although the BHSA does not specifically reference the CHA and only the CHIP, the CHA and CHIP are part of the same local LHJ planning process, and the CHA is the essential precursor step to developing the CHIP.
-
Informed by the CHA, the CHIP identifies how the public health entity will work with community partners to address key issues elevated in the CHA.
An array of tools and processes may be used to conduct a CHA and develop a CHIP; the essential feature is that these processes are informed by community collaboration and participation. Since the CHA and CHIP processes are tailored to address local community needs, there is no requirement to include prescribed topic areas such as specialty or non-specialty mental health, or other content areas.
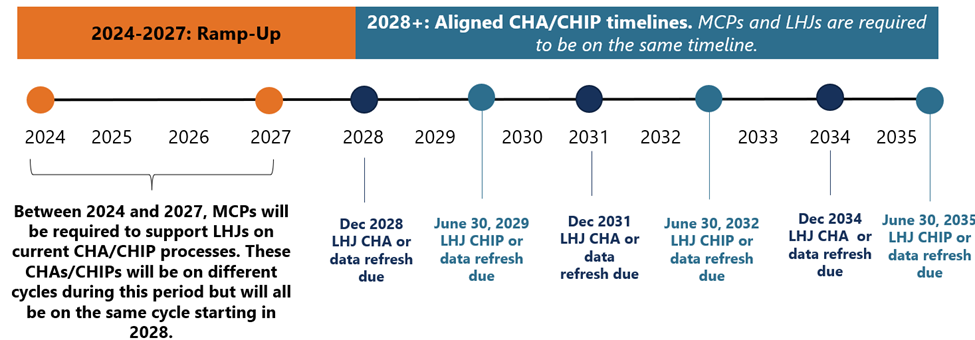
At present, most LHJs complete or update their CHAs and CHIPs every five years when seeking to obtain and maintain voluntary Public Health Accreditation Board (PHAB) accreditation. Some LHJs are on a three-year submission cycle to align with local processes, such as non-profit hospital community health needs assessments. Currently, non-accredited LHJs can choose not to formally conduct CHAs and CHIPs.
Starting in 2028, as a part of the collaborative state efforts to improve local integration in community planning, the CHA and CHIP will be mandatory for all LHJs, and all LHJs will implement the same three-year submission cycle, as described below in Figure 3.B.2.1. This timeline is intentionally designed to align with and inform BHT IP planning processes as well as simplify the new local planning policy for MCPs operating in multiple local health jurisdiction areas.
B.2.1.2 Background: MCP PNA
Historically, the PNA has been the mechanism that MCPs use to identify (1) priority needs of their local communities and members and (2) health disparities. Under the CalAIM Population Health Management (PHM) Program, since January 1, 2024, MCPs have fulfilled their PNA requirement by meaningfully participating in the development of LHJ CHAs and CHIPs in the service areas where MCPs operate. As noted above, the term “local planning” is now used to describe these new requirements.
MCP meaningful participation includes:
-
Collaboration. MCPs must participate in every LHJ CHA and CHIP in their service area and collaborate with other MCPs within the same service areas to foster a unified planning process.
-
Data-Sharing. MCPs are expected to share data with LHJs in ways that support the CHA and CHIP process.
-
Stakeholder Engagement. MCPs must attend key CHA and CHIP meetings and serve on CHA and CHIP governance structures, as requested by LHJs.
-
Funding and/or In-Kind Staffing. Starting on January 1, 2025, MCPs are required to contribute funding and/or in-kind staffing to support LHJ CHA and CHIP processes.
See the CalAIM PHM Policy Guide for additional details on MCP local planning Requirements (pages 7-10).
MCPs are required to submit a PHM Strategy which provides details on MCPs’ meaningful participation on LHJs’ CHA and CHIP.
DHCS and CDPH collaborated to create a regulatory environment that supports effective and efficient joint work on CHAs and CHIPs between LHJs and MCPs. Thus, aligned with CDPH guidance, the cycles for LHJs’ CHA and CHIP development will become standardized across California starting in 2028, as previously noted, and as displayed in the timeline below.
B.2.2 Overlap and Alignment with Other Local Program Planning Processes
County behavioral health departments (counties), LHJs, and MCPs share a common interest in identifying the needs of the populations and communities they serve. Points of integration existed before SB 326 and its IP mandate, and some counties, LHJs, and MCPs have been collaborating on CHA/CHIP processes for many years.
Specific to BHSA mandates that counties work with MCPs and LHJs on CHAs and CHIPs, DHCS has established the following guiding principles to work toward the achievement of common goals:
-
Counties, LHJs, and MCPs serve overlapping local communities and should collectively be aware of key, population-level needs and challenges.
-
There is an opportunity to employ complementary and coordinated strategies and interventions across delivery systems.
-
As counties begin to engage in the CHA and CHIP processes, alignment should lead to more integrated, upstream, and effective community health initiatives and prevention strategies to improve population health.
-
Given the distinct focus areas and different populations that LHJs, MCPs, and counties serve, DHCS intends for this alignment to supplement the broader county IP requirements.
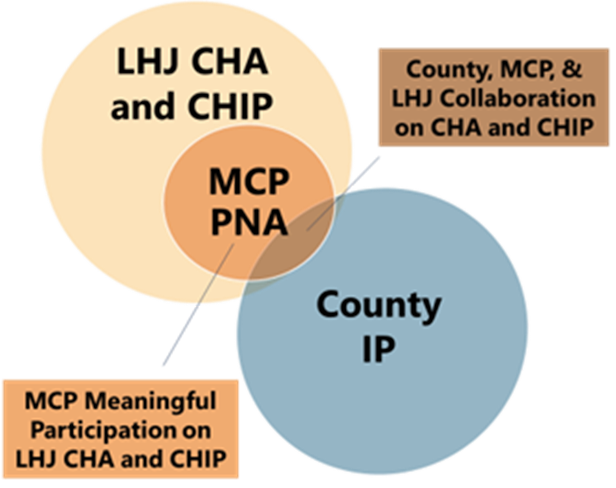
Figure 3.B.2.2 depicts the initial level of overlap anticipated as counties and LHJs embark on, or in some cases continue, collaborative efforts related to the development and alignment of community needs assessments and planning processes. Additionally, it demonstrates that the IP has numerous requirements unrelated to the LHJ CHA and CHIP. However, over time, as relationships advance, collaboration strengthens, and timelines align, county, MCP, and LHJ overlap on CHAs and CHIPs will likely increase, and the overlap in these circles will expand.
B.2.3 County Requirements
This section provides county requirements, effective January 2025, for alignment with LHJs and MCPs in support of the IP submissions.
-
Engagement with Other Local Program Planning Processes
Counties are required to engage with LHJs and MCPs on CHAs and CHIPs, across the three areas described below. However, given that counties’ IPs and LHJs’ CHAs and CHIPs are driven by unique local needs, DHCS will allow for flexibility in how counties may work with LHJs and MCPs. For example, specific behavioral health topics and focus areas may vary from county to county.
Area 1: Collaboration. Over time, counties, LHJs, and MCPs can partner to focus on coordinated strategies for upstream interventions that can improve population health. To advance meaningful collaboration, counties are required to:
-
Work with LHJs on the development of the CHA and CHIP in that county (or city, recognizing three city LHJs. For a complete list of LHJs, see CDPH’s listing of local health services/offices.), along with MCPs, in fulfillment of their meaningful participation requirements. If multiple MCPs are present in the county or city, they will already be aligned in support of the LHJ in accordance with DHCS PHM Policy Guide mandates.
-
Attend key CHA and CHIP meetings and serve on CHA and CHIP governance structures, including CHA and CHIP subcommittees, at the request of LHJs when discussions are relevant to behavioral health issues.
Area 2: Data-Sharing. Counties, LHJs, and MCPs all have access to their own siloed data. When this data is shared among these partners, it can be used to improve population health by creating a more holistic picture of the multiple factors contributing to a community’s health. Counties are expected to work with LHJs and MCPs to determine the types of relevant data to be shared, taking into consideration the specific nature of CHAs and CHIPs, and the needs of the counties, and how data should be de-identified/disaggregated. Counties are required to begin to identify Statewide Behavioral Health Goals (as described in Chapter 2, Section C.2 Statewide Population Behavioral Health Goals) to:
-
Share aggregate and deidentified data to support behavioral health related focus areas of the CHA/CHIP. Counties, LHJs, and MCPs are sometimes hesitant to share data given their perceived or real concerns that federal and/or state law restricts them from doing so. However, both HIPAA and 42 CFR Part 2 permit the disclosure of properly deidentified data for public health purposes, including community-level planning activities that support statewide behavioral health objectives.
-
Utilize and stratify data from LHJs and MCPs to inform IP development.
Counties are subject to various and specific mandates regarding data sources, uses, and stratification for IP development that exceed the integration of LHJs’ and MCPs’ data. DHCS expects that counties must continue to meet any broader data requirements required by the IP that may not be fulfilled through the LHJ CHA and CHIP processes.
Area 3: Stakeholder Engagement. Given that BHSA identifies more than twenty specific populations and stakeholder groups that counties must engage in the development of the IP, counties should work with LHJs to look for opportunities where IP stakeholder engagement could be combined or integrated with CHA/CHIP processes to reduce duplication and community fatigue. LHJs generally involve a wide array of community stakeholders in the CHA and CHIP development processes. In order to streamline community input and reduce redundancy, counties are required to:
-
Coordinate stakeholder activities for IP development with LHJ engagement on the CHA and CHIP to the extent possible.
-
Consider input from diverse populations and a wide range of community stakeholders.
DHCS expects that counties must continue to meet any broader stakeholder engagement requirements that may not be fulfilled through the LHJ CHA and CHIP processes.
Because LHJ stakeholder engagement on CHAs and CHIPs is uniquely focused on the individual needs of each community, there are no prescribed topics or mandated focus areas. However, behavioral health may be a key focus area identified by communities. Counties are expected to participate in the CHA and CHIP as described above, and where behavioral health-specific needs arise through the progress, work with LHJs and MCPs to incorporate addressing such needs in its IP.
The county requirements across all three areas noted mirror MCP requirements for meaningful participation on LHJs’ CHAs and CHIPs. DHCS does not require or expect counties to provide funding and/or in-kind staffing to support the LHJ CHA and CHIP processes. Per the CalAIM: PHM Policy Guide, however, MCPs are required to work with LHJs to determine what combination of funding and/or in-kind staffing the MCP will contribute to the LHJ CHA/CHIP process.
As mentioned previously, due to the current disparate submission cycles for LHJ CHAs and CHIPs, counties should consider the most recent CHA and CHIP on record, which could be up to four years old (depending on the submission cycle) and/or may not be available in all LHJs, when preparing their 2026 IP submissions. For the LHJs without CHAs or CHIPs available, counties should reach out to their respective LHJ to determine if a Strategic Plan is available for their review.
-
Technical Assistance: Local Planning Collaboration Toolkit
To support successful partnerships among counties, LHJs, and MCPs, DHCS has developed a 2025 – 2026 BHSA Local Planning Collaboration Toolkit. This tool may be used to support collaboration, data sharing, and stakeholder engagement.
Additionally, DHCS will engage LHJs separately to provide their insight on the collaboration with counties.
-
Iterative Approach for Overlap and Alignment
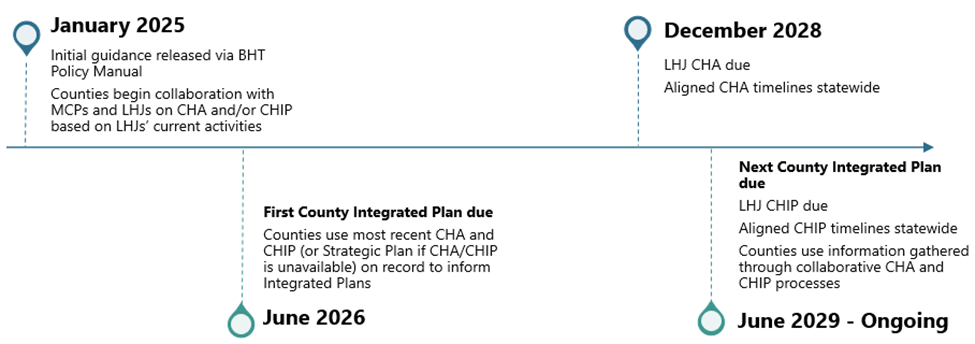
Figure 3.B.2.3 below details the timeline for implementation of the county, LHJ, and MCP collaboration requirements for the first IP submission in 2026 through the 2029 IP submission.
Counties, LHJs, and MCPs should take time in 2025 to come to a common understanding of the respective key facts, goals, and language in each system.
-
Opportunities should be identified for each entity to share background on their respective requirements and processes (relative to the IP, the PNA, and the CHAs and CHIPs) and how they utilize these tools.
-
Counties, MCPs, and LHJs should ensure all parties are aligned on one another’s roles and responsibilities, the populations they serve, and the services they are responsible for providing.
B.3 Public Comment and Updates to the Integrated Plan
Comment Period
Counties are required to provide 30 days for stakeholder comment on each IP. An IP and update shall be prepared and circulated for review and comment for at least 30 days (WIC section 5963.03, subdivision (a)(2)(B)) to representatives of stakeholder interests and any interested party who has requested a copy of the plans.
Local Behavioral Health Board
The local behavioral health board shall conduct a public hearing on the IP at the close of the 30-day comment period (WIC section 5963.03, subdivision (b)(1)).
Once an IP is ready for public comment, the local behavioral health board is required to review the draft plan and make recommendations to the local behavioral health agency for revisions (WIC section 5963.03, subdivision (b)(4)). The local behavioral health board is not required to approve county Integrated Plans.
The local behavioral health agency is also required to provide an annual report to the local governing body (WIC section 5963.03, subdivision (b)(5)), which is the local Board of Supervisors or city council, and DHCS that includes written explanations in response to any substantive recommendations made by the local behavioral health board that are not included in the final IP or update (WIC section 5963.03, subdivision (b)(5)).
Revisions to the Integrated Plan
After the 30-day comment period and public hearing are complete, counties are required to make the following revisions to the IP:
-
Each IP should include a summary of substantive written recommendations (WIC section 5963.03, subdivision (b)(2)).
-
The IP should also include a summary and analysis of the revisions made as a result of stakeholder feedback (WIC section 5963.03, subdivision (b)(3)).
Annual Updates and Intermittent Updates
Counties must prepare AUs to their IP and may prepare IUs, although IUs are not required. When preparing AUs or IUs, counties are encouraged, but not required, to comply with the stakeholder process outlined in WIC section 5963.03, subdivision (a) and WIC section 5963.03, subdivision (b). Counties may choose to elicit participation from stakeholders when preparing AUs and IUs. If counties choose to request stakeholder feedback through the formal community planning process, the county must comply with the local behavioral health board public hearing requirements (WIC section 5963.03) outlined above.
Counties must post AUs and IUs to their IP and a summary and justification of changes to their website for a 30-day comment period prior to the effective date of the updates (WIC section 5963.03, subdivision (c)(2)(B)). Counties can download their completed IP from the county portal and submit to the Behavioral Health Services Oversight and Accountability Commission (BHSOAC).
B.4 County Planning Funds
B.4.1 Planning Costs
Counties may allocate up to 5 percent of the total annual revenue received from the local Behavioral Health Services Fund (BHSF) to fund planning costs. All allocations and expenditures for planning costs must be included in the county IP and Behavioral Health Outcomes Accountability and Transparency Report (BHOATR). These planning costs (WIC section 5892, subdivision (c)) shall include funds for county mental health and substance use disorder programs to pay for the costs of consumers, family members, and other stakeholders to participate in the planning process.
Planning costs may be used to help pay for infrastructure and technologies that will support robust stakeholder engagement. Examples may include but are not limited to:
-
Laptops and other technologies to help stakeholders participate in the planning process
-
Web-based meeting platforms
-
Virtual engagement tools
-
Accessibility services
-
Stipends, wages, and contracts to be paid to consumers and family members
-
Translation/interpretation services
-
Travel and transportation for stakeholders
-
Childcare
-
Eldercare
-
Training and technical assistance (TTA) for stakeholders to be meaningfully involved including TTA on fiscal policies
-
Other supports to help with stakeholder engagement
Counties may use planning funds to assess public behavioral health workforce needs required as part of the IP, including the number of providers and vacancies in the county, the county’s ability to develop and maintain a robust workforce that provides adequate access to services and supports, and address statewide behavioral health goals described in Chapter 2, Section C of this policy manual. Counties will no longer be required to submit a separate Workforce Needs Assessment beyond what is included in the IP.
Planning costs do not include costs incurred as administrative costs or program expenditures. Additional information on administrative costs, including direct and indirect costs, can be found in Chapter 6.B.
C. Behavioral Health Care Continuum
C.1 Background
Each county’s Integrated Plan (IP) and its associated budget template is required to describe how it will spend behavioral health dollars across a care continuum. Specifically, each county is required to demonstrate, per WIC section 5963, subdivision (a)(1), how it will:
“utilize various funds for behavioral health services to deliver high quality, culturally responsive, and timely care along the continuum of services in the least restrictive setting from prevention and wellness in schools and other settings to community-based outpatient care, residential care, crisis care, acute care, and housing services and supports.”
To provide counties with more specificity as to what it means to provide care along “the continuum of services,” the California Department of Health Care Services (DHCS) has defined a Behavioral Health Care Continuum. The Behavioral Health Care Continuum is composed of two distinct frameworks for substance use disorder (SUD) and mental health (MH) services. These frameworks will allow counties to describe their expenditures across key service categories, identify gaps in their service continuum, and articulate the investments they will make to expand access, close identified gaps, and improve performance as indicated through statewide behavioral health goals. The use of a standardized Behavioral Health Care Continuum also enables state-level analysis and comparison over time and across counties. The information that counties provide through the Behavioral Health Care Continuum in the IP will not be used to evaluate compliance with expenditure requirements for Behavioral Health Service Act (BHSA) funds.
C.2 Behavioral Health Care Continuum
Counties will report on planned service delivery and expenditures in the IP and budget template, and actual service delivery and expenditures in the Behavioral Health Outcomes, Accountability, and Transparency Report (BHOATR) and expenditure template, disaggregated by child/youth under age 21 and adults aged 21 and older, within the Behavioral Health Care Continuum service categories outlined below.
Counties will plan expenditures in the IP by totaling the dollar amount across all behavioral health funding streams for each Behavioral Health Care Continuum service category and will report actual expenditures in the BHOATR by listing the dollar amount from each behavioral health funding stream for each Behavioral Health Care Continuum service category.
The Behavioral Health Care Continuum (shown in Figure 3.C.1) has eight service categories across discrete SUD and MH frameworks, which capture behavioral health programs and services delivered by county behavioral health agencies. The SUD framework includes services provided in facilities designated as Institutions for Mental Disease (IMD) and services in non-IMD facilities. The Behavioral Health Continuum includes services provided in facilities designated as IMDs and services in non-IMD facilities. The IMD exclusion is only applicable to billing for Medi-Cal services. SUD services referenced in Figure 3.C.1 reflect the American Society of Addiction Medicine (ASAM) 3rd Edition; Medi-Cal guidance on ASAM 4th edition is forthcoming.
One category, Housing Intervention Services, will be reported as a single total across the SUD and MH frameworks within the IP. For the BHOATR, DHCS will ask counties to report actual spending on Housing Intervention Services distinctly in each of the SUD and MH frameworks.

The Behavioral Health Care Continuum does not include county expenditures on: 1) workforce investment activities; 2) capital infrastructure activities; 3) quality and accountability, data analytics, plan management, and administrative activities; and 4) other non-clinical service county behavioral health agency activities (e.g. Public Guardian, forensic activities, Community Assistance, Recovery and Empowerment (CARE) Act). Counties will report these expenditures in the IP and BHOATR distinctly from the Behavioral Health Care Continuum. These non-Continuum expenditure categories will be described in forthcoming guidance on IP and BHOATR reporting.
Tables 3.C.1 and 3.C.2 below describe each of the categories that span the SUD and MH frameworks. The tables below offer descriptions of each service category – informed by DHCS's previous assessment of California's Medi-Cal behavioral health service delivery system and tailored to the county landscape – as well as examples of the specific services that should be reported under the SUD and MH frameworks. A more detailed inventory cataloguing DHCS’ recommended approach to reporting service expenditures across categories in the Behavioral Health Care Continuum will be provided with the release of the IP and BHOATR. Some services, like peer supports, medication services, and case management, may cut across several categories in the Behavioral Health Care Continuum; the funding for these services should be allocated according to the setting in which services are delivered (i.e., peer support services delivered within an outpatient setting should be categorized within “outpatient services”).
SUD and MH frameworks include county reporting on population prevention services. While DHCS recognizes BHSA funds for population prevention are exclusively with the California Department of Public Health (CDPH), counties have other funds that they may use for population prevention (e.g., Substance Abuse and Mental Health Services Administration (SAMHSA) Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG), opioid settlement, Realignment, etc.) which DHCS anticipates this category will capture.
Table 3.C.1 Substance Use Disorder Care Continuum Service Categories, Definitions, and Example Services
|
Service Categories |
Service Category Definition |
Example SUD Services (ASAM 3rd edition) |
|
Population Prevention Services |
Includes services and activities that educate and support individuals to prevent substance misuse and substance use disorders from developing. These services/activities offer communities support in identifying and addressing issues, tools for coping with stressors and information on ways to promote resiliency. They may also include services and public health campaigns focused on overdose prevention. Note: BHSA funds for population prevention are exclusively with the California Department of Public Health. |
|
|
Early Intervention Services
|
Includes interventions that take a proactive approach to identifying and addressing substance use issues among individuals who are showing early signs, or are at risk, of a substance use disorder. These interventions, such as outreach, access and linkage, and treatment services, help avert the development of a severe and disabling condition, discourage risky behaviors and support individuals in maintaining healthy lifestyles. |
|
|
Outpatient Services
|
Includes a variety of therapeutic substance use disorder services that can be provided anywhere an individual is located, such as in school, home, clinic, office, or other outpatient settings. These services may help avert the need for, or be provided after, crisis care, inpatient, or residential treatment. These services are provided, if necessary, as part of stabilization and continued recovery/ongoing evaluation. |
|
|
Intensive Outpatient Services |
Includes services to support individuals living with higher acuity SUD needs who may require assistance at a higher frequency and/or intensity, sometimes via a team-based approach. These services offer structure and monitoring when more support than routine outpatient visits is necessary. |
|
|
Crisis and Field-Based Services |
Includes a range of services that engage, assess, stabilize, treat, and/or coordinate care for individuals in need of substance use disorder services in field settings (e.g., homeless encampments, shelters, or syringe service programs). Services may be delivered in non-traditional settings where individuals work or reside. |
|
|
Residential Treatment Services |
Includes low- to high-intensity clinically managed residential treatment. Services may be delivered in short-term residential settings of any size. |
|
|
Inpatient Services |
Includes 24-hour, intensive treatment services to individuals who require medical management or medical monitoring for substance use disorder needs. |
|
|
Housing Intervention Services (reporting is aggregated with the mental health framework) |
Includes services and supports designed to enable individuals to remain in their homes or obtain housing to support recovery and improved health outcomes. Services help individuals find and retain housing, support recovery and resiliency, and/or maximize the ability to live in the community. |
|
Table 3.C.2 Mental Health Care Continuum Service Categories, Definitions, and Example Services
|
Service Categories |
Service Category Definition |
Example MH Services |
|
Population Prevention Services |
Includes services and activities that educate and support individuals to prevent acute or chronic conditions related to mental health from ever developing. These services/activities may offer communities support in identifying and addressing issues before they turn into problems, tools for coping with stressors and information on ways to promote resiliency. |
|
|
Early Intervention Services
|
Includes interventions that take a proactive approach to identifying and addressing mental health issues among individuals who are showing early signs, or are at risk, of a mental health disorder. These interventions, such as outreach, access and linkage, and treatment services, help avert the development of a severe and disabling condition, discourage risky behaviors and support individuals in maintaining healthy lifestyles. |
|
|
Outpatient & Intensive Outpatient Services
|
Includes a variety of therapeutic mental health services that can be provided anywhere an individual is located, such as in school, home, clinic, office, field settings (e.g. homeless encampments, shelters, etc.) or other outpatient settings. Also includes services to support individuals living with higher acuity mental health needs who may require assistance at a higher frequency and/or intensity, sometimes via a team-based approach. These services may help avert the need for, or be provided after, crisis care, inpatient or residential treatment and are provided, if necessary, as part of stabilization and continued recovery/ongoing evaluation. They may also offer structure and monitoring when more support than routine outpatient visits is necessary. |
|
|
Crisis Services |
Includes a range of services and supports that assess, stabilize, and treat individuals experiencing acute distress. Services are designed to provide relief to individuals experiencing a mental health crisis, including through de-escalation and stabilization techniques, and may be delivered in clinical and non-clinical settings. |
|
|
Residential Treatment Services |
Includes intensive treatment services that are provided in a structured, facility-based setting to individuals who require consistent monitoring for mental health needs on a longer-term basis. Services may be delivered in short-term residential settings to divert individuals from or as a step-down from hospital and acute services. |
|
|
Hospital and Acute Services |
Includes treatment services that are provided in structured, hospital settings to individuals who require consistent monitoring and stabilization. These services may include comprehensive psychiatric treatment, including medication adjustments, and acute withdrawal services. |
|
|
Subacute and Long-Term Care Services |
Includes intensive licensed skilled nursing care provided to patients with mental health needs, most frequently delivered in a skilled nursing facility (SNF) and special treatment programs (STPs). |
|
|
Housing Intervention Services (reporting is aggregated with the substance use disorder framework) |
Includes services and supports designed to enable individuals to remain in their homes or obtain housing to support recovery and improved health outcomes. Services help individuals find and retain housing, support recovery and resiliency, and/or maximize the ability to live in the community. |
|
D. County Integrated Plan Alignment with Statewide Population Behavioral Health Goals
As outlined in WIC section 5963.02, subdivision (c)(3)(A), each county shall develop an Integrated Plan (IP) and annual update (AU) aligned with their associated measures. DHCS will identify and provide counties with measures of their performance relative to the statewide behavioral health goals. Counties will use those measures to inform resource planning in their IPs and AUs, as well as their approach to population health management and implementation of targeted interventions to drive progress on statewide behavioral health goals. In forthcoming guidance, DHCS will describe its approach to calculating performance measures and delineate expectations for counties, MCPs, and other stakeholders as part of a monitoring and accountability framework. See Chapter 2, Section C for more detailed information.
E. Guidance for Completing the Integrated Plan
E.1 Integrated Plan Template
The Integrated Plan template and budget template are provided as separate documents.
E.2 General Requirements
E.2.1 Integrated Plan Requirements
E.2.1.1 Draft Integrated Plan Requirements
All counties must submit a draft Integrated Plan (IP) by March 31 of the fiscal year prior to the fiscal years covered in the IP to the Department of Health Care Services (DHCS). All exemption or funding transfer requests must be submitted as part of the draft IP submission.
Counties must also include a letter from the County Administrator approving the draft IP, including the exemption and funding transfer request, within the draft IP submission. The County Administrator may be known by other titles such as Chief Executive, County Manager, or Chief Administrative Officer. The County Administrator must be the individual who serves as the top staff member in county government and hold the highest level of administrative authority in the county or be the designee of that individual. This individual or their designee must work within the executive office of county government, and they may not be the county behavioral health director.
In the IP, counties are required to report all planned activities for county behavioral health services provided under the funding sources listed in Chapter 3, Section A.2 of the Behavioral Health Services Act (BHSA) County Policy Manual. Counties are required to report planned expenditures for the activities and services reported in the IP in an accompanying budget template, described further in Chapter 3, Section E.2.2. below. DHCS will provide close-ended response options (e.g., yes/no questions, multiple-selection buttons, dropdown menus, or numerical responses) where possible to promote consistency and data analysis across county IPs.
To complete the IP and project estimates for the plan period, counties must refer to relevant data from the most recent sources available (WIC section 5963.02, subdivision (b)(2)) or from the dates specified by DHCS in the IP template. DHCS recognizes that some information required in the IP, particularly regarding population-level health and demographics, may change during the time period covered by the IP or annual update. The purpose of requiring such information in the IP is to provide background information on the county and the county’s behavioral health delivery system that can be leveraged by counties and stakeholders during the community planning process.
For a draft IP to be considered complete, a county must include the following:
-
Response to each required item in the IP template.
-
Include certifications from both the county behavioral health director and the County Administration Officer (or other county equivalent) or their designee certifying compliance with fiscal accountability requirements and that all planned expenditures are consistent with applicable state and federal law (WIC section 5963.02, subdivision (c)(11)).
In order to have IPs that are effective July 1, DHCS anticipates that the draft IP submitted will be as close to final as possible, with minimal changes to the final IP submission.
E.2.1.2 Final Integrated Plan Requirements
IPs and annual updates are required to be circulated for a 30-day comment period. Counties may choose whether to circulate their IP before or after they submit their draft IP; however, it must occur prior to submitting the final IP.
Then, after completing the 30-day public comment period, counties must submit their IP to the local behavioral health board for review. The behavioral health board must conduct a public hearing on the IP. The behavioral health board then must review the IP or update and make recommendations for revisions (WIC section 5963.03, subdivision (b)(4)).
Counties must also receive approval from the county Board of Supervisors and certification from the county behavioral health director, before submitting the final IP to DHCS by June 30 of the fiscal year prior to the fiscal years covered in the IP (WIC section 5963.02, subdivision (a)(3)).
For a final IP to be considered complete, a county must include the following:
-
Response to each required item in the IP template.
-
Include certification from the county behavioral health director, ensuring that the county has complied with all pertinent regulations, laws, and statutes (WIC section 5963.02, subdivision (c)(10))all applicable regulations, laws, and statutes.
-
Include certification by the county Board of Supervisors attesting the county will meet its realignment obligations (WIC section 14197.71, subdivision (c)(2)).
E.2.2 Budget Template Requirements
In the IP budget template, counties must report all planned behavioral health service expenditures for each funding source listed in Chapter 3, Section A.2 according to the Behavioral Health Care Continuum categories outlined in Chapter 3, Section C.2 of the Policy Manual. The planned expenditures included in the budget template must align with the services and activities the county reports in the IP.
In the “BH CC Expenditures” tab of the budget template, counties will total the dollar amount across the required behavioral health funding streams for each Behavioral Health Care Continuum service category (both Substance Use Disorder (SUD) and Mental Health (MH) frameworks), disaggregated by children/youth under age 21 and adults aged 21 and older. One category, Housing Intervention Services, will be reported as a single total across the SUD and MH frameworks within the IP. For the Behavioral Health Outcomes, Accountability, and Transparency Report (BHOATR), DHCS will ask counties to report actual spending on Housing Intervention Services distinctly in the SUD and MH frameworks. The information provided in the “BH CC Expenditures” tab of the IP budget template will not be used to evaluate compliance with expenditure requirements for the Behavioral Health Service Act (BHSA) funds.
The Behavioral Health Care Continuum does not include projected expenditures for:
-
Workforce investment activities
-
Capital infrastructure activities
-
Quality and accountability, data analytics, plan management, and administrative activities
-
Other county behavioral health agency activities not otherwise captured in the Care Continuum (e.g. Public Guardian, LPS Conservatorship, DSH for housing, court diversion programs, Community Assistance, Recovery and Empowerment (CARE) Act)
Counties will report these expenditures separately in the “Other County Expenditures” tab of the budget template.
In addition to reporting expenditures according to the Behavioral Health Care Continuum, counties must report projected expenditures for each BHSA program component – Housing Interventions, Full Service Partnership (FSP) and Behavioral Health Services and Supports (BHSS) – in the respective tabs of the budget template. Counties will report BHSA administration costs that are directly related to each of the BHSA components within each component tab. Administrative costs that are associated with implementing the new requirements under BHSA should be included in the BHSA Plan Admin tab of the budget template. BHIN 25-016 provides instructions on how to claim reimbursement for the new requirements. Detailed instructions for reporting projected expenditures for each BHSA program component are included in the respective tabs.
Counties must also report projected total behavioral health expenditures, BHSA component exemptions and transfers, plan administration expenditures, and prudent reserve assessments in accordance with the instructions provided in the budget template.
E.3 Process for Requesting Exemptions
E.3.1 Eligible Exemptions
Counties, if eligible, are allowed to request exemptions from some requirements for the BHSA Housing Interventions and FSP components. (All counties, regardless of population size, will be exempt from certain FSP requirements for the FYs 2026-2029 IP.) Please see Chapter 7, Section C.6.2 for information regarding Housing Intervention exemptions and Chapter 7, Section B.3.4 FSP Exemptions for information regarding FSP exemptions. For information about funding transfers, please see Chapter 6, Section B.4.
E.3.2 Exemptions Submission
Counties, if eligible, requesting an exemption from Housing Intervention and/or FSP requirements must submit the request through the county portal as part of the draft IP by March 31 of the fiscal year prior to the fiscal year covered in the IP (i.e., exemption requests for the 2026-2029 IP must be submitted to DHCS by March 31, 2026). Counties must begin their community planning process prior to submitting an exemption request to determine local priorities to make the exemption requests responsive to local needs. Exemption requests are only valid for the duration of the three-year plan. For each subsequent three-year plan submission, counties must submit updated exemption requests for DHCS approval.
E.3.3 Acceptance Criteria
DHCS will review the information provided in the county’s IP and determine whether the exemption request aligns with the exemption criteria outlined in the Policy Manual. Counties requesting an exemption to either increase or decrease the required funding allocations for Housing Intervention programs must provide information that meets the criteria for Housing Intervention exemption requests in Chapter 7, Section C.6.2. Counties requesting one or more FSP exemption must provide information that meets the criteria for FSP exemption requests in Chapter 7, Section B.3.4.
E.3.4 Exemptions Approval
DHCS has 30 calendar days from receipt of the exemption request to approve or deny the county’s request for exemption (WIC section 5892, subdivision (a)(1)(B)). The approval and/or denial of the exemption request will be completed through the county portal. If DHCS does not respond within 30 calendar days, the exemption request will be considered approved (WIC section 5892, subdivision (a)(1)(B)).
E.3.5 Appeals Process
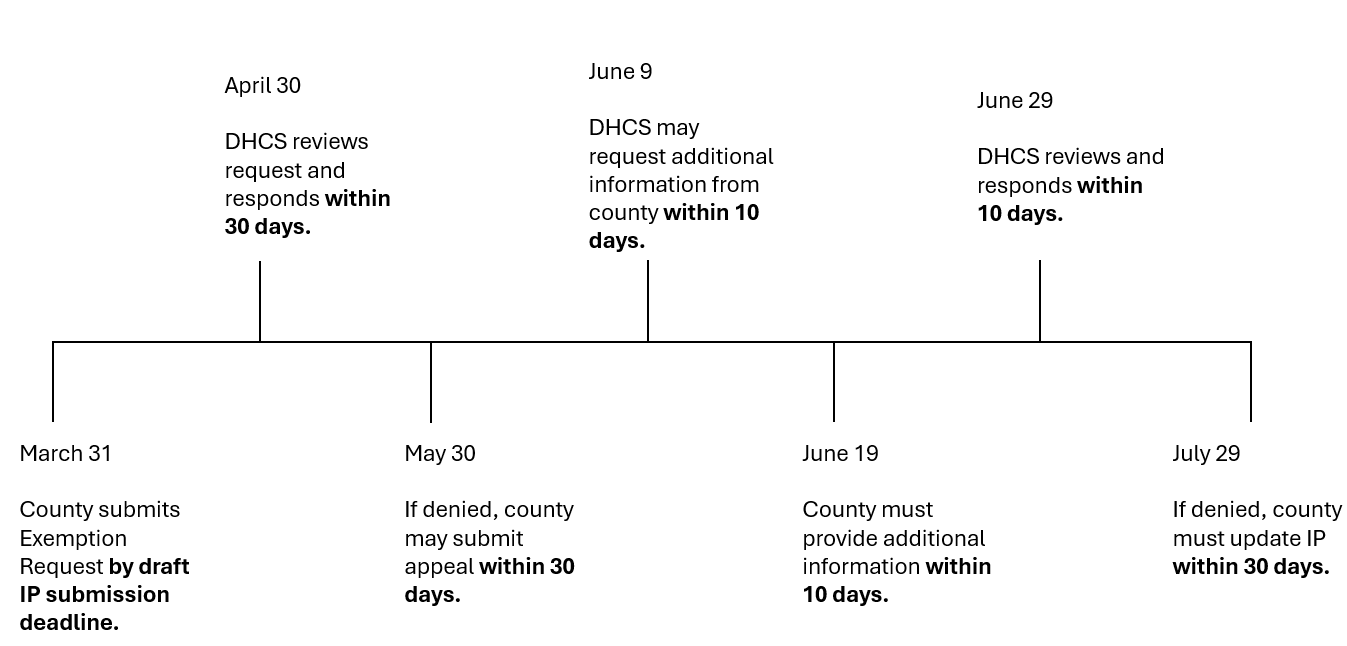
Counties may appeal DHCS’ decision to deny the county’s exemption request. All appeals activities will occur through the county portal. Counties must submit their appeal request within 30 calendar days of receiving DHCS’ denial. The appeal must include an explanation stating the basis of the appeal and supporting documentation. DHCS has 30 calendar days to approve or deny the appeal, starting with the date that DHCS confirmed receipt of the appeal. If an appeal is submitted after 30 calendar days from receipt of the denial, the appeal will be automatically denied.
DHCS will have 10 calendar days from confirming receipt of the appeal to request additional documentation from the county; counties will supply additional documentation within 10 calendar days of confirming receipt of the request. DHCS will review and approve or deny the request within 10 calendar days of receiving the county’s additional documentation. If DHCS rejects the exemption requested in the county’s IP, the county must update their IP to reflect the denied exemption in their IP by June 30th of the year prior to the fiscal years the IP covers.
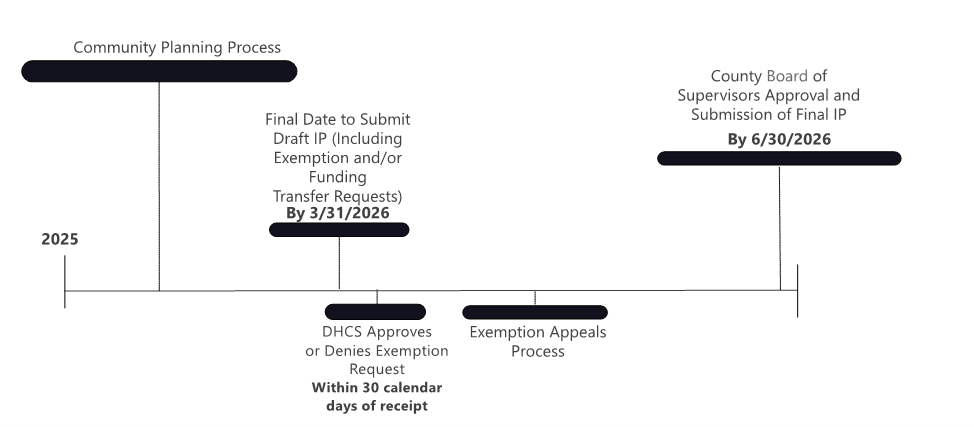
Exemption Appeals Process and Timeline:
-
County submits Exemption Request with the draft IP by March 31 deadline.
-
DHCS reviews request and approves or denies within 30 calendar days of request receipt.
-
If denied, county may submit an appeal through the county Portal within 30 calendar days of DHCS’ decision.
-
DHCS may request additional documentation from the county within 10 calendar days of receipt of the appeal.
-
The county must respond to DHCS’ documentation request within 10 calendar days of DHCS’ request.
-
DHCS will review and approve or deny within 10 calendar days of receiving the additional documentation.
-
If the request is denied, DHCS will provide a justification for the denial and the county must update their IP by June 30th of the year prior to the fiscal years the IP covers.
E.4 Integrated Plan Submission
A final IP is due no later than June 30. County board of supervisor approval is required for submission by June 30 prior to the fiscal year the IP will cover. County Board of Supervisor approval (WIC section 5963.02, subdivision (a)(3)) of the first IP is due by June 30, 2026; this IP will cover fiscal years 2026-2029. Please refer to Figure E.2.1, the 2026-2029 Integrated Plan Submission Timeline, to see deadlines for the first IP.
Counties must also use the county portal to submit questions or concerns about IP submission and approval or for technical assistance with the submission.
Counties that fail to submit their IP by the March 31 and June 30 deadlines are out of compliance and may be subject to corrective action. DHCS’ BHSA oversight policies will be discussed in future BHSA Policy Manual modules.
E.4.1 County Portal
Counties will develop and submit their IPs online through the DHCS county portal and may do so on a rolling basis once the county portal is publicly available. The county portal will include technical features that will increase transparency and give DHCS and stakeholders greater insight into the IP development process. The county portal will allow county users to complete tasks such as filling in form-based prompts, documenting stakeholder involvement requirements, compiling fiscal information, and completing attestations. The county portal will support access for multiple county users, allowing multiple county teams to work concurrently to develop the IP. Counties must also use the county portal to submit questions or concerns about IP submission and approval or for technical assistance with the submission.
County portal technical features will include progress markers to track completion of each section of the IP, support tools allowing DHCS staff to review, collaborate on, and resolve questions from counties, and functionalities to distill key information into county profiles, which can show stakeholders where their county is in the community planning and IP development process. DHCS staff will be able to concurrently review county IP submissions and communicate directly with county contacts to resolve questions. The county portal will track both the county’s progress in completing IP sections, DHCS staff review progress in a dashboard view, and for communication with counties about their plans.
E.4.2 DHCS Review Standards
DHCS will review a county’s draft and final IP for completeness and validate that all IP content is aligned with guidance set forth in this Policy Manual and all BHSA statutory requirements. Upon submission, questions that require close-ended response options or document uploads will be automatically reviewed for completeness in the county portal. Line items in the budget template will be automatically validated where possible to ensure expenditures align with fiscal requirements outlined in this Policy Manual. DHCS staff will review IP submissions to ensure they include but are not limited to:
-
Sufficient rationale for any requested exemptions or funding transfers (submitted with draft IP by March 31 for review of exemption and funding transfers).
o Rationale for Housing Interventions or Full Service Partnerships (FSP) exemption requests must align with exemption criteria as described in Chapter 7, Section C.6 and Chapter 7, Section B.3.4 of this Policy Manual.
-
Narrative content to ensure responses adequately address questions.
-
Documentation of a complete community planning process and public comment period as described in Chapter 3, Section B of this Policy Manual.
-
Goals for Population Behavioral Health measures and behavioral health disparities that are consistent with statewide behavioral health goals outlined in Chapter 2, Section C and Chapter 3, Section D of this Policy Manual and forthcoming related guidance.
-
Projected expenditures and service utilization estimates across the Behavioral Health Care Continuum as described in Chapter 3, Section C of this Policy Manual.
-
Projected BHSA component transfers, exemptions, and expenditure plans, BHSA administrative expenditures, prudent reserve information, and other county expenditures as outlined in the budget template and budget instructions.
Additionally, all proposed uses of behavioral health funding in the IP must be consistent with allowable expenditures for FSP, Housing Interventions, and Behavioral Health Services and Supports (BHSS). A complete IP must include a response to each required item in the county portal.
Table E.4.1 Submission Requirements for Draft and Final Integrated Plan
|
|
Draft Integrated Plan |
Final Integrated Plan |
|
Deadline |
By March 31, 2026 |
By June 30, 2026 |
|
Activities required prior to submission |
Engage stakeholders through the local CPP |
|
|
Items required to be included with submission |
|
|
County responses may be flagged for further review by DHCS monitoring divisions for follow-up regarding compliance issues. This is not a punitive process, rather an opportunity for DHCS to reach out to counties and assess whether technical assistance or other support may be needed, or to recommend revisions to the county’s plan to align proposed activities with state guidance.
DHCS may require counties to revise their IP if DHCS determines the IP or annual update fails to adequately address the following local needs, as outlined in statute (WIC section 5963.02, subdivision (b)(2)):
-
Prevalence of mental health and substance use disorder.
-
Unmet need for mental health and substance use disorder treatment in the county.
-
Behavioral health disparities.
-
Homelessness point-in-time count.
-
Allocation of funding between mental health and substance use disorder treatment services.
DHCS will review draft and final IPs for completeness and adherence to policy requirements prescribed in the Policy Manual and statute within 30 calendar days of submission. If DHCS deems a county’s IP or annual update does not address a question directly or is inaccurate, DHCS will contact the county through the county portal to rectify and resubmit the IP as described in Chapter 3, Section E.2 of this Policy Manual. DHCS will contact all the county primary and secondary contacts listed in the IP submission to rectify and resubmit the IP. If DHCS requests the county revise their draft IP, the county will have 15 calendar days from the revision notice to address the issues raised by DHCS and resubmit the IP through the county portal. Counties are not required to undergo the stakeholder engagement process to resubmit their IP. DHCS will review the revised IP and respond through the county portal within 15 calendar days. IPs are effective beginning July 1 of the fiscal year the IP covers, and counties should move forward with their IP beginning July 1, even if the county is in the process of providing additional information to DHCS. Once the revised IP is resubmitted, DHCS will review the IP according to the criteria outlined in this section.
Submission for annual and intermittent updates will follow the same process as outlined above for the county IP. DHCS will review changes to the IP included in the annual and intermittent update as appropriate. Counties do not need to resubmit sections of the IP that have not changed in intermittent updates.
E.5 Joint Submission for Local Entities
This section describes the process for two or more county behavioral health departments acting jointly, or one or more city-operated programs or departments acting jointly with another city-operated program or department or county behavioral health department to submit a joint IP.
E.5.1 Submission Process
Counties that submitted joint three-year plans under the Mental Health Services Act (MHSA) (WIC section 5897, subdivision (b)) may continue to submit joint IPs under BHSA; the two city-operated mental health authorities receiving funds pursuant to WIC section 5701.5 shall submit IPs independently from their counties under BHSA. Counties that have separate mental health and substance use disorder departments are required to collaborate on development of the IP and submit one joint IP to their county Board of Supervisors.
E.5.2 Guidance for Joint Integrated Plan Completion
Entities that submit joint IPs should complete the IP and IP budget template to report all planned activities and projected expenditures for all behavioral health services provided by the entities that are part of the joint powers authority (GOV section 56047.7) or joint submission. Counties with separate mental health and SUD departments must also report all planned activities and projected expenditures for BHSA services. The planned activities and projected expenditures must be reported as a combined total in accordance with the budget template for all entities included in the joint powers authority, joint submission, or the multiple county departments submitting jointly. Entities submitting a joint IP must ensure that data in the IP is unduplicated, including number of eligible individuals, individuals served, and services provided.
Counties must consider input and feedback provided by stakeholders (WIC section 5963.02, subdivision (b)(8)) to develop their IP; counties that submit joint IPs must engage stakeholders from all counties included in the joint submission. Counties (including joint powers authorities and counties submitting a joint IP under another arrangement) that have a combined total population greater than 200,000 are required to engage with the five most populous cities in the county (WIC section 5963.02, subdivision (b)(7)) as part of the community planning process. Cities submitting IPs independently will not need to collaborate with other cities. Counties (including joint powers authorities and counties submitting a joint IP under another arrangement) and cities submitting IPs independently are subject to the population threshold requirements outlined in this Policy Manual related to fiscal requirements (Chapter 6, Section B) and FSP and Housing Interventions (Chapter 7, Section B.3.4 and Chapter 7, Section C.6.2, respectively) exemptions.
E.5.3 Approval Process for Joint Integrated Plans
The IP must be approved by the Board of Supervisors for each county represented in the joint IP or other local governing body prior to final submission to the Behavioral Health Services Oversight and Accountability Commission (BHSOAC) and DHCS. Joint IP submissions must include certification from the joint entity’s behavioral health director as described in Chapter 3, Section 3.E.2.
E.6 Statewide Behavioral Health Goals
DHCS, in consultation with behavioral health stakeholders and subject matter experts, identified 14 statewide behavioral health goals focused on improving wellbeing and decreasing adverse outcomes. These behavioral health goals will inform state and county planning and prioritization of resources, and DHCS will continuously assess statewide and county progress toward these goals.
Counties must refer to the statewide behavioral health goals and associated measures during the county BHSA planning process. In their IP, counties are required to address the actions they are taking on seven required goals, including six priority goals and at least one goal in which the county-wide data is higher or lower than the statewide rate or average, as appropriate:
-
Access to Care
-
Homelessness
-
Institutionalization
-
Justice-involvement
-
Removal of children from home
-
Untreated behavioral health conditions
-
County/City/Joint Powers Authority-selected goal (from the remaining eight statewide behavioral health goals)
Counties may select more than one additional statewide behavioral health goal. Planning for each goal must be informed by the measures and reflect an approach for improving overall performance on the goal and for addressing disparities.
For the first IP due by June 30, 2026, each county reviewed data for all population-level behavioral health measures (i.e., Phase 1 measures) to inform their planning. For the population-health measures used only in the first IP, DHCS identified “primary” and “supplemental” population-level behavioral health measures (referred to as primary measures and supplemental measures).
-
Primary measures reflect the community’s status and wellbeing for each goal, as defined in the Policy Manual. There is one primary measure (or a pair of related primary measures) for each goal.
-
Supplemental measures provide additional context and data that are useful to better understand the status of the goal and inform planning. There are up to two supplemental measures for each goal.
The population-level behavioral health measures used for the first IP can be accessed in the County Population Behavioral Health Measure Workbook.
For all IPs, IUs, and AUs submitted after July 1, 2026, each county must use the performance measures, as listed in Chapter 2, Section C.3, to inform planning on the statewide behavioral health goals.